Effective Obturation Techniques for Successful Root Canal Treatments

Root canal treatment is a routine yet crucial procedure in dental practice, involving several precise steps to ensure long-term success. Among these steps, obturation stands out as one of the most important because properly sealing the root canal prevents reinfection and promotes healing over the years. While many dentists rely on the familiar and straightforward cold lateral compaction method, there are several other obturation techniques worth knowing—and practicing—to achieve better clinical outcomes. In this blog, we’ll explore these different methods, helping you expand your knowledge and refine your skills for more predictable and successful root canal treatments.
What is Obturation?
According to the American Association of Endodontists, “Obturation is the method used to fill and seal a cleaned and shaped root canal using a root canal sealer and core filling material.”
The main purpose of obturation is to eliminate all portals of entry between the periodontium and the root canal. The better the seal, the better the prognosis of the root canal.
Read Also: Manual vs Rotary Endodontics: A Comprehensive Comparison for Successful Root Canal Treatment
Different Types of Obturation Materials:
- Silver Cones: Silver cones are no longer recommended in endodontic practice as they start corroding when they come into contact with saliva or periradicular fluids, and the by-products are highly toxic.
- Gutta-Percha: It is the most commonly used solid core filling material in endodontics. It is a trans-isomer of polyisoprene and exists in alpha and beta crystalline forms. The material is solid in the beta phase and does not shrink. On heating, the beta phase changes into the alpha phase, which is tacky and flowable under pressure. Due to the poor sealing property of gutta-percha, regardless of technique, it must be combined with a root canal cement or sealer to ensure proper filling and sealing of the root canal.
- Resilon: It is a high-performance polyurethane introduced recently as an alternative to gutta-percha. This system can be placed using lateral compaction, warm vertical compaction, or thermoplastic injection. However, long-term clinical trials are needed before completely replacing gutta-percha with this material.
- MTA: Mineral trioxide aggregate (MTA) can be used as a canal obturation material because of its superior physiochemical and bioactive properties. However, retreatment of canals filled with MTA is quite difficult. Also, there is a potential for discoloration when used in the anterior esthetic zone.
Different Techniques of Obturations:
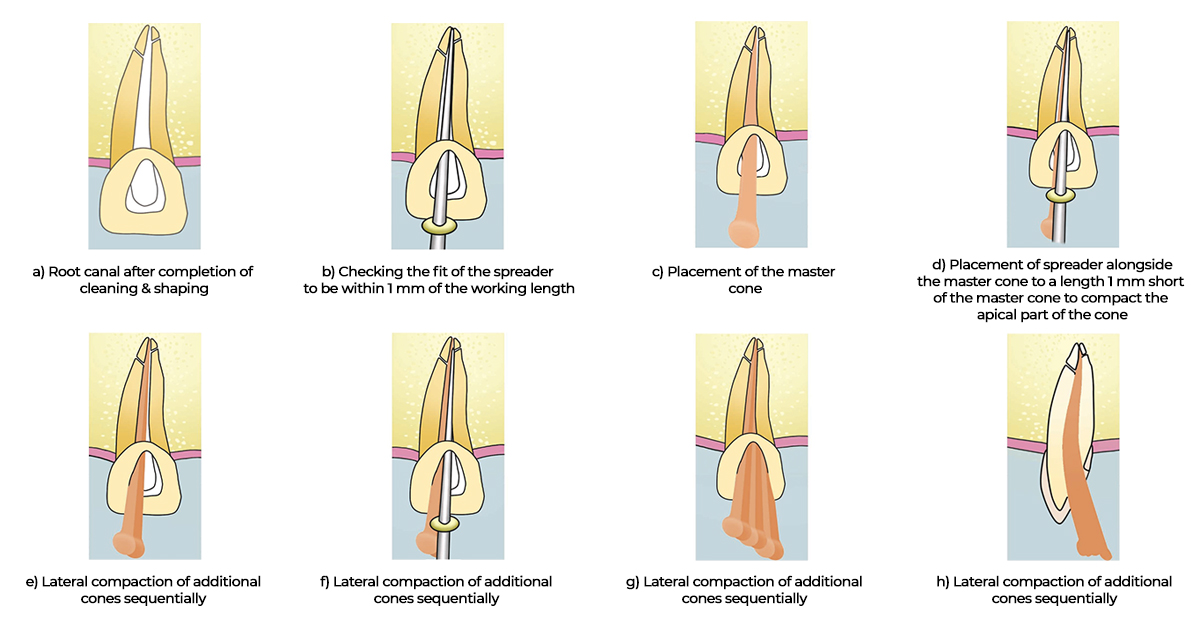
1. Cold Lateral Compaction Obturation Technique:
It is the most commonly used technique by dentists all over the world. However, it is still not the best technique to achieve a three-dimensional seal. The cold lateral technique basically involves the selection of the size of the spreader based on the width of the prepared canal and the lateral fit of the primary cone. The fit of the primary cone is verified by radiograph. The fit of the spreader should be within 1 mm of the working length. This is followed by the placement of the master cone. The spreader is then again placed alongside the master cone to a length 1 mm short of the master cone to compact the apical part of the cone.
Similarly, lateral compaction of the additional cones is done sequentially until the spreader cannot be reinserted—an indication that the root canal is fully compacted laterally. Several radiographs must be taken while one obturates the canal to check the accuracy of the procedure, and only after thorough verification should the post-obturation restoration be done.
Limitations:
- Presence of voids in the filling
- Increased sealer:GP ratio when compared with thermoplasticized techniques
- Not as effective in sealing intracanal defects and lateral canals when compared to warm compaction techniques
2. Warm Compaction (warm gutta-percha) Obturation Technique:
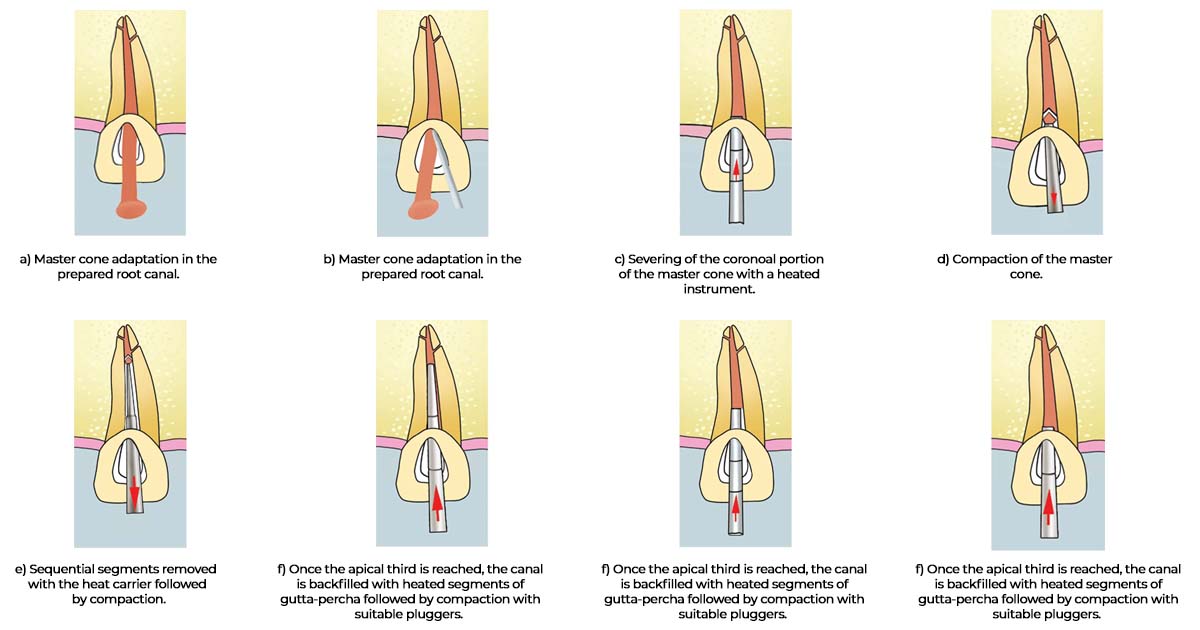
(a) Warm Vertical Compaction–
The main principle of this technique is to fill the root canals as well as the lateral and accessory canals with heat-softened gutta-percha. A heated plugger is used to apply pressure in a vertical direction, causing the gutta-percha to flow and fill the entire lumen of the canal. The step-by-step procedure can be appreciated in the diagram below.
Limitations:
- Time-consuming procedure
- Risk of vertical root fracture resulting from undue force
- Possibility of overfilling with gutta-percha or sealer, which cannot be retrieved from the periradicular tissues
(b) Warm Lateral Compaction –
The warm lateral compaction involves the placement of the master cone and lateral compaction using heat carriers, thus providing the advantages of the thermoplasticized technique as well as length control during obturation. The device is placed beside the master cone and activated, followed by the placement of an unheated spreader in the space previously occupied by the heat carrier. Accessory cones are then placed, and the process is repeated until the canal is filled.
Top Recommendations: EndoKing Obturation Pen , SuperEndo Dental Buchanan Hand Pluggers
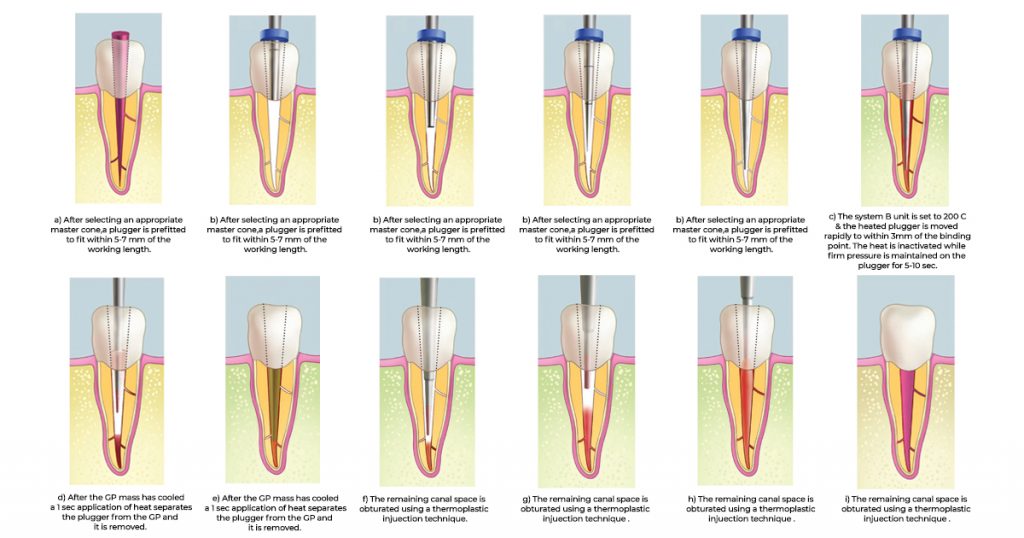
3. Continuous Wave Compaction Obturation Technique:
Introduced by Buchanan, this technique is a variation of warm vertical compaction. It requires the use of gutta-percha cones and pluggers that mimic the tapered preparation, thereby permitting the application of greater hydraulic force during warm compaction. It uses tapered nickel-titanium systems to prepare the canal. Pluggers are selected in accordance with the shaping instruments used. Tapered pluggers with sizes #.06, #.08, #.10, and #.12 are used, with tip diameters similar to the tapered gutta-percha points. The procedure is carried out with a heat carrier system.
The step-by-step procedure can be appreciated in the diagram below.
Top Recommendation: Endoking ObturaPro Obturation System
4. Thermoplasticized Gutta-Percha Injection Obturation Technique:
This technique involves the use of a pressure apparatus, more commonly called an Obturation Gun, consisting of an insulated electrically heated syringe barrel and a selection of needles ranging from 18 to 25 gauge size. The canal is prepared similarly to any other technique, and sealer is coated after drying the canal. The system allows adequate heating of the gutta-percha pellets, and a suitable gauge needle is selected to be positioned 3–5 mm short of the working length. Gutta-percha is gradually injected by squeezing the trigger of the gun, and the needle is gradually withdrawn as the canal gets filled apically. The gutta-percha is then compacted using pluggers of appropriate size. The rest of the canal can be filled in one to two increments in the same way.
When practicing the injection method, it is recommended that the canal preparation is restricted apically, with flaring of the body of the canal toward the access opening to minimize the flow of the gutta-percha.
Limitations:
- Lack of precision apically can often lead to the flow of gutta-percha.
- The interface seal between the gutta-percha and the canal wall is weak, and voids occur in the final set filling.
Top Recommendation: Woodpecker Obturation Gun
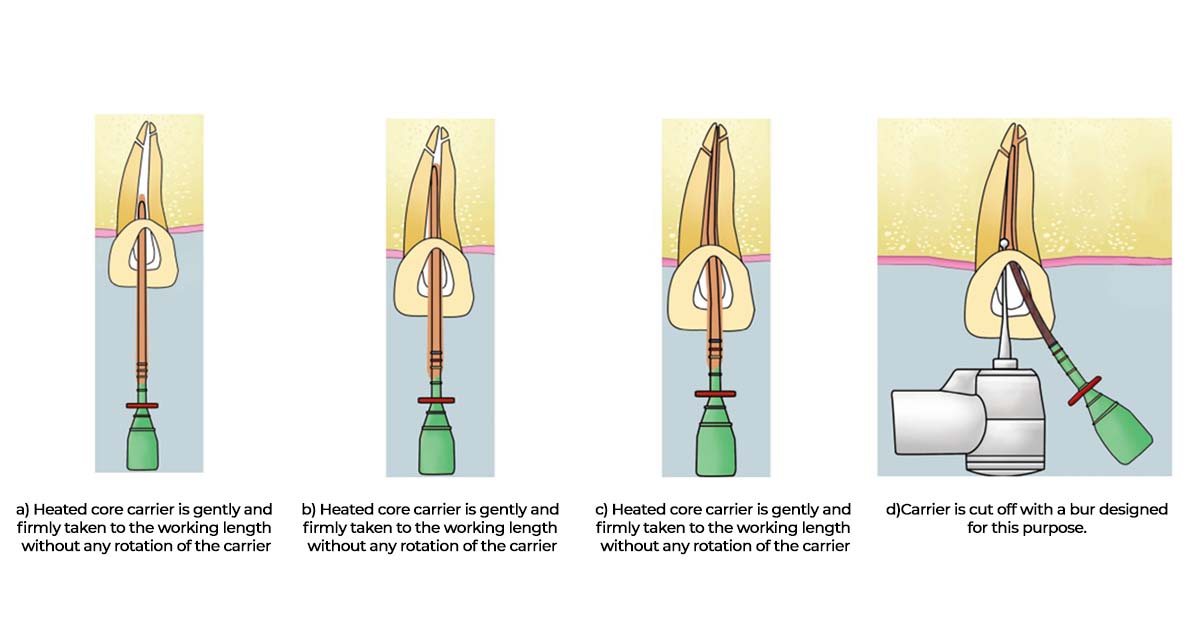
5. Carrier-based Gutta-Percha Obturation Technique:
(a) Thermafil Thermoplasticized –
The Thermafil is a carrier-based gutta-percha obturation system comprising a plastic core carrier coated with alpha phase gutta-percha. These Thermafils are available in ISO standardized sizes as well as tapered sizes for canals prepared with NiTi tapered instruments.
After the canal is prepared, the size is verified with a Thermafil verifier instrument, which helps in the selection of the appropriately sized obturator. Drying of the canal followed by sealant application is done as in any other technique. The silicon stopper on the carrier is adjusted to the working length, and the carrier is loaded into the Thermaprep plus Oven device for approximately 10 seconds. The carrier is then inserted into the canal and placed up to the working length with firm, uniform apical pressure without rotating. The position of the carrier is verified radiographically, and the gutta-percha is allowed to cool for 2–4 minutes before resecting the carrier at the level of the canal orifice.

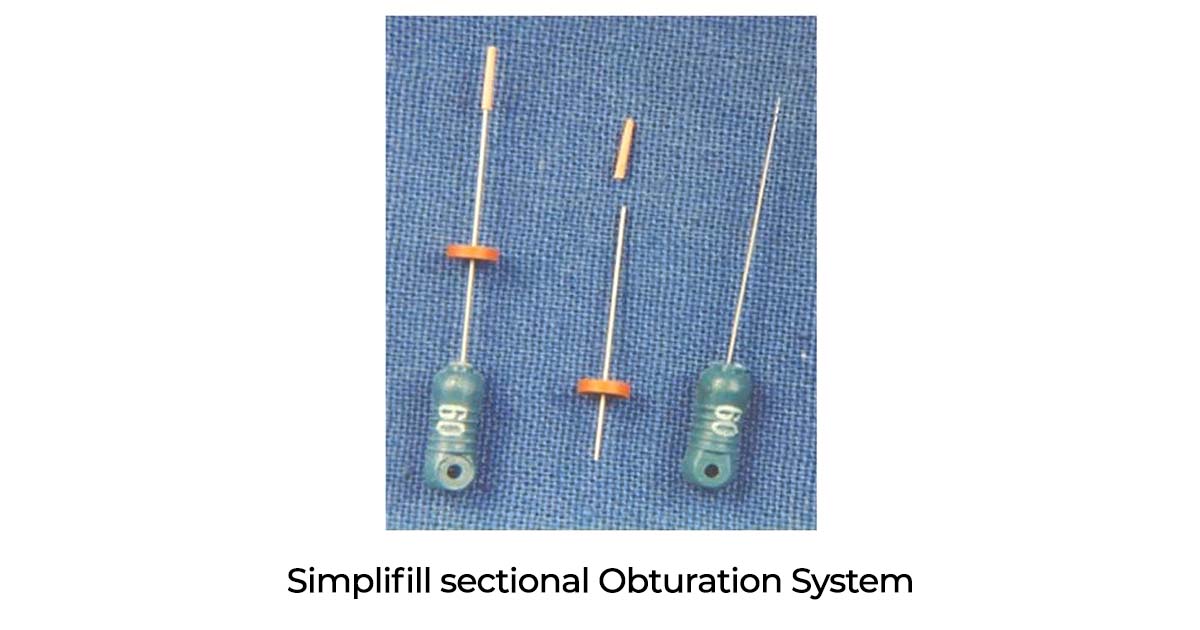
(b) SimpliFill Sectional Obturation –
It is a carrier-based sectional gutta-percha obturation system used in conjunction with light-speed rotary instruments. The SimpliFill carrier has an apical 5 mm plug of gutta-percha, which performs cold sectional obturation of the root canal. After the usual drying and sealant application in the canal, the carrier is selected depending on the master apical file and introduced up to the working length. The handle of the carrier is rotated quickly in the counterclockwise direction three to four times to disengage the apical plug of gutta-percha from the carrier. The remaining coronal space can be filled with lateral compaction or thermoplasticized gutta-percha methods.
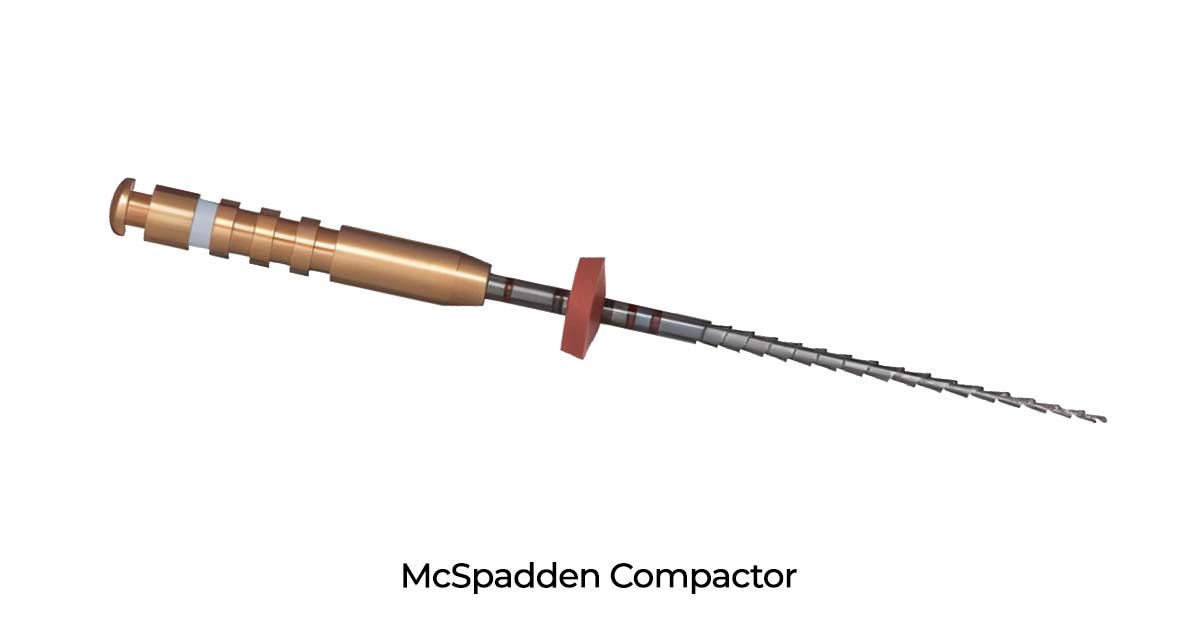
6. McSpadden Thermomechanical Compaction Obturation Technique:
Introduced by McSpadden, this technique uses heat to decrease the viscosity of gutta-percha and increase its plasticity. The heat is created by rotating a compacting instrument in a slow-speed contra-angle handpiece at 8,000–10,000 RPM alongside gutta-percha cones inside the root canal. The stop on the compactor blade helps guide the rotating tip of the blade to within 1.5 mm of the root apex, helping prevent gutta-percha from flowing beyond the apex. The compactor, whose spiraled 90° flutes are similar to the flutes on a Hedstroem file but in reverse, forces the softened gutta-percha apically and laterally.
Disadvantages:
- Cannot be used in narrow canals
- Compactor blades often break in the canal
- Frequent overfilling of the canal
- Shrinkage of the cooled or set filling
7. Chemically Plasticized Gutta-Percha Obturation Technique:
This technique is no longer recommended. It involves gutta-percha being plasticized with chemical solvents like chloroform, eucalyptol, or xylol. The disadvantage of using a chemical-solvent filling material is its inability to control overfilling, often leading to periapical tissue reaction and shrinkage of the filling after setting, resulting in a poor apical and lateral seal.
8. Custom Cone Obturation Technique:
It is a chair-side procedure wherein the dentist customizes the cone for adequate tug-back in a canal. The technique involves softening the gutta-percha with one or more accessory cones using heat or rolling between two glass slabs to achieve a single master cone of the required size. Another method is softening the master gutta-percha with chloroform, eucalyptol, or halothane for a few seconds and gently placing it to the working length with a locking plier. Upon removal, the softened gutta-percha has the impression of the canal, and this process is repeated until a snug fit is achieved.
Conclusion:
In summary, successful root canal treatment relies heavily on effective obturation, which involves sealing the canal to prevent reinfection. While cold lateral compaction remains widely used, exploring other techniques such as warm compaction, continuous wave, thermoplasticized injection, carrier-based systems, and thermomechanical compaction can significantly improve sealing quality and clinical outcomes. Each method has its advantages and limitations, making it essential for clinicians to understand and select the best approach based on individual case requirements. Embracing these advanced techniques not only enhances treatment success but also helps you stay at the forefront of endodontic practice. For all your dental materials and equipment needs to implement these methods efficiently, explore Dentalkart—your reliable partner in dental innovation and supplies.
No Comment