Dental Ergonomics: Posture, Chair Positioning, and Four-Handed Dentistry

Dental Ergonomics for Dentists: Posture, Chair Positioning, and Four-Handed Dentistry – Dentistry demands precision, focus, and often long hours in static positions — all of which can take a serious toll on the body if proper ergonomics are ignored. Poor posture and awkward positioning can lead to chronic neck, back, and shoulder pain, ultimately affecting both performance and long-term health.
That’s why understanding and applying the right dental ergonomics is essential for every dental professional. From correct sitting posture and patient positioning to ideal operating zones and instrument handling, this blog covers everything you need to work efficiently and stay pain-free.
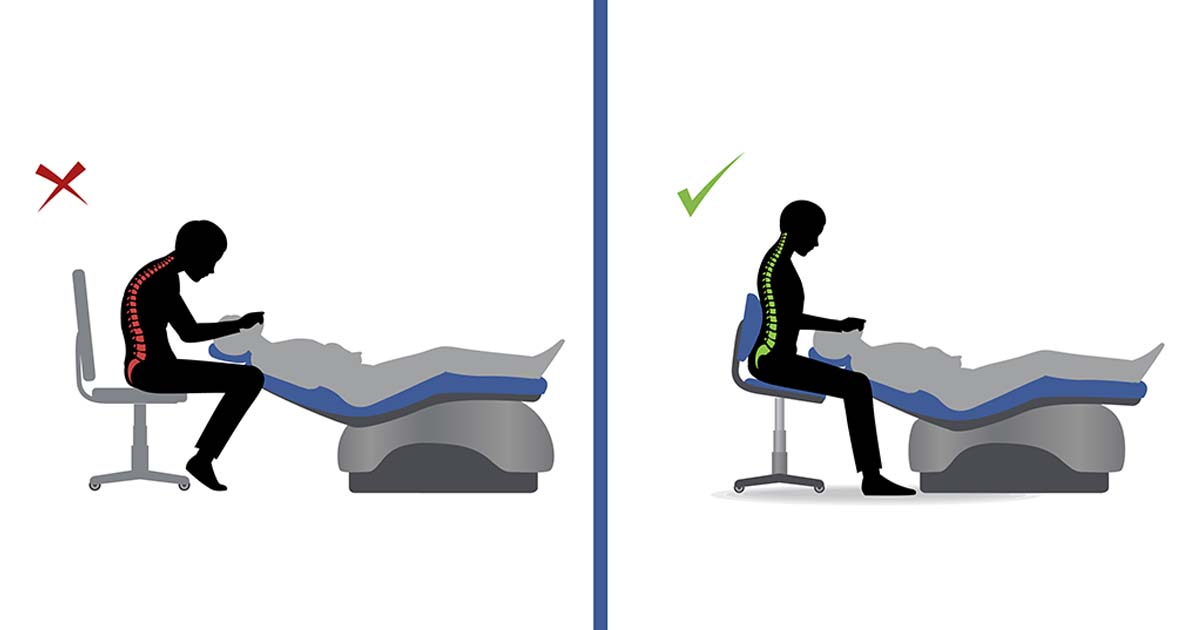
The Ideal Posture that should be followed:
- Head: The head should be inclined slightly forward, oriented over the shoulders. The interpupillary line should be aligned horizontally at 15 to 20 degrees.
- Torso: The torso should be upright to promote the natural curvature of the spine. The backrest of the chair can be positioned to provide lumbar support if needed.
- Upper arms, elbows, and shoulders: The arms should be relaxed on one side, elbows should not stick out, forearms should be in front, and shoulders oriented over the hips.
- Wrists: They should be kept straight in a neutral position.
- Fingertips: They should be aligned so that they don’t obstruct the site of operation and should grip the instrument correctly.
- Seated posture: Seating height should be similar to knee height, with hips slightly higher than the knees. One can tilt the stool slightly forward.
- Feet: The feet should be flat on the floor with knees vertically placed.
- Rheostat/Foot pedal positioning: It should be placed closer to the operator so that the knee is at about 90-100 degrees. If placed farther, the dentist might have to slouch to the other side, ultimately leading to back and neck strain.
Read Also: Ergonomics in Dentistry: Avoiding Occupational Risks
Patient Positioning:
The right patient positioning should be determined according to the dentist’s natural posture and their reference point, allowing him/her to achieve optimal performance without physical strain. The right patient and operator’s position help in the welfare of both individuals. A patient seated comfortably is more relaxed, has less muscle tension, and cooperates better with the dentist.
Most dental procedures are done in a seated position except for a few. Any uncomfortable or unnatural position should be avoided when positioning a patient, whether for standing or seated position of the operator during the procedure. A dental chair should provide full body support to the patient in any position. The chair usually has an adjustable headrest which helps in resting the patient’s head; contoured chairs further help with adequate support. Most chairs are programmable and can be adjusted with just a button at the dentist’s instrument platform on the chair.
We will now discuss the operating positions that should be followed by dentists in detail:
Operating Positions:
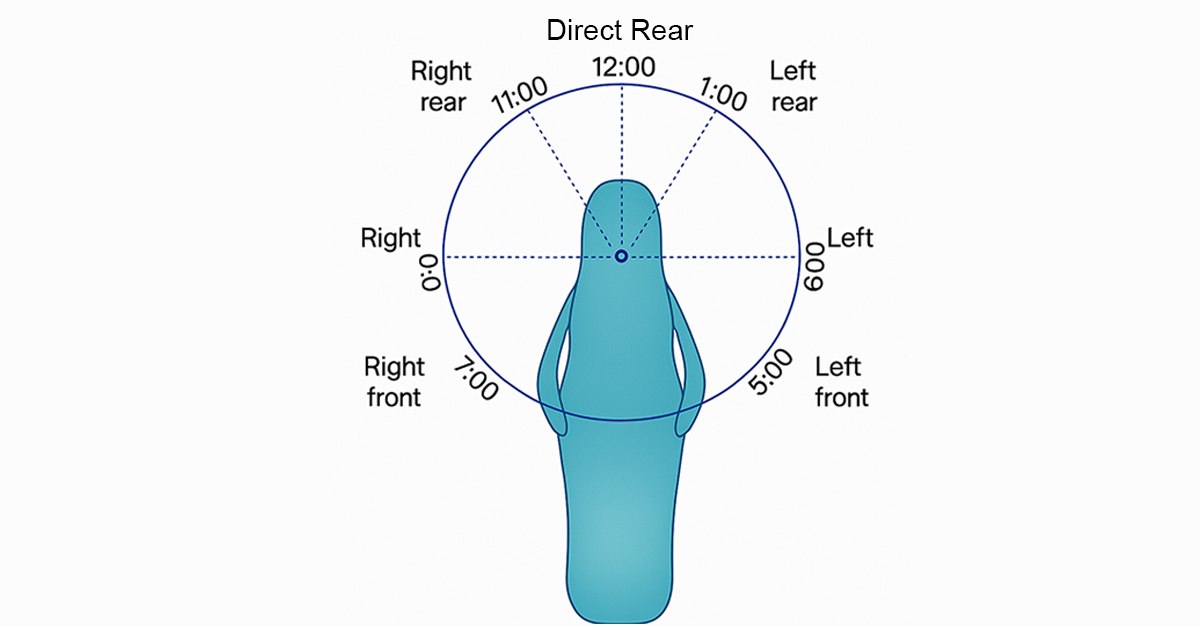
The operating positions are usually described according to the location of the operator or by the location of the operator’s arms in relation to the patient’s position.
- A right-handed dentist mostly uses three positions:
a. Right front, also known as the 7 o’clock position
b. Right, also known as the 9 o’clock position
c. Right rear, also known as the 11 o’clock position
- A left-handed operator uses the following positions:
a. Left front, also known as the 5 o’clock position
b. Left, also known as the 3 o’clock position
c. Left rear, also known as the 1 o’clock position
- Another position often used is the direct rear position, or the 12 o’clock position. As a rule, the teeth being treated should be at the same level as the operator’s elbow.
The operating positions described below are for right-handed operators; left-handed operators can substitute the same accordingly, as it is mostly on the exact opposite side compared to a right-handed dentist.
Right Front Position:
This position helps in the examination and treatment of mandibular anterior teeth, mandibular posterior teeth (especially on the right side), and maxillary anterior teeth. It is often advised to have the patient’s head tilted towards the operator.
Right Position:
In the right position, the operator is directly to the right of the patient. This position is helpful for operating on the facial surfaces of maxillary and mandibular right posterior teeth and the occlusal surfaces of mandibular right posterior teeth.
Right Rear Position:
In this position, the operator is behind and slightly to the right of the patient. The left arm is positioned around the patient’s head. When operating from this position, the lingual and incisal (occlusal) surfaces of the maxillary teeth are viewed using the mouth mirror. Left mandibular teeth are in direct vision, but the use of a mouth mirror is advocated for visibility, light reflection, and retraction.
Direct Rear Position:
This positioning is used for operating on the lingual surfaces of mandibular anterior teeth. The operator is located directly behind the patient and looks down over the patient’s head.
Procedure-wise recommended Chair Positions:
| Procedure | Chair Position | Description of Chair Setup |
|---|---|---|
| Routine Check-ups and Cleanings | Slightly reclined (45-60°) | The patient is reclined at a moderate angle for easy access to the teeth. The headrest should be adjusted to align with the dentist’s working position (usually supine). |
| Tooth Extractions (Non-surgical) | Fully reclined (90°) | Patient should be fully reclined for maximal access to both upper and lower teeth. The headrest is slightly tilted back to keep the head in a neutral position. |
| Tooth Extractions (Surgical) | Fully reclined, slight head tilt backward (30-45° tilt) | For maxillary extractions, headrest should be angled backward slightly (for good access to upper teeth). For mandibular extractions, the angle can stay more flat. This helps the operator to access the site easily. |
| Root Canal Treatments | Fully reclined (90°), slight head tilt downward (10-20°) | This is for good visibility, especially for anterior or posterior root canals. The patient’s head should be slightly tilted down for better access to the root of the tooth. |
| Implant Placement | Fully reclined (90°), head tilted slightly backward (15-30°) | For implant surgeries, a fully reclined position ensures access to both upper and lower jaw. Slight tilt of the head backward is ideal for maxillary implants. |
| Fillings and Crowns | Slightly reclined (45-60°) | This position allows for easy access to anterior or posterior teeth. A moderate recline provides comfort for the patient and enables the dentist to easily access the area of concern. |
| Periodontal Scaling and Root Planing | Slightly reclined (45-60°) | A moderate recline helps the dentist access the gums, particularly for lower posterior teeth. The headrest should be slightly angled for optimal access to the treatment area. |
| Orthodontic Adjustments | Slightly reclined (30-45°) | A slight recline is often preferred for orthodontic procedures to keep the patient comfortable while working on the upper or lower jaw. The angle ensures easy access to both anterior and posterior teeth. |
| Endodontic Treatment | Fully reclined (90°), head tilted slightly downward (10-15°) | Similar to root canal treatment, but with a slight tilt of the head downward for access to anterior or posterior teeth. This is especially helpful for visibility and precision during cleaning and shaping of canals. |
| Soft Tissue Surgery | Fully reclined, head tilted slightly backward (20-30°) | For surgical procedures involving soft tissues, such as gingival flaps, the chair should be fully reclined to maximize access to the treatment area. A slight backward tilt of the head allows better visibility and control. |
| Frenectomy (or other soft tissue removal) | Fully reclined (90°), head tilted slightly back (15-20°) | The full recline with a slight backward tilt provides optimal access to the oral cavity, especially for upper lip or lower gum line procedures. |
| Oral Surgery (Cysts, Tumors, Biopsy) | Fully reclined (90°), head tilted back (30-45°) | Full recline allows for the best visibility, especially for oral biopsies, cyst or tumor removal, or impacted tooth extractions. The head tilt helps in reaching the upper arch. |
| Pediatric Dentistry | Slightly reclined or upright (30-45°) | Children often require the chair in an upright position for comfort and security. For procedures like fillings or exams, a slight recline is used for comfort. |
Four-Handed Dentistry:
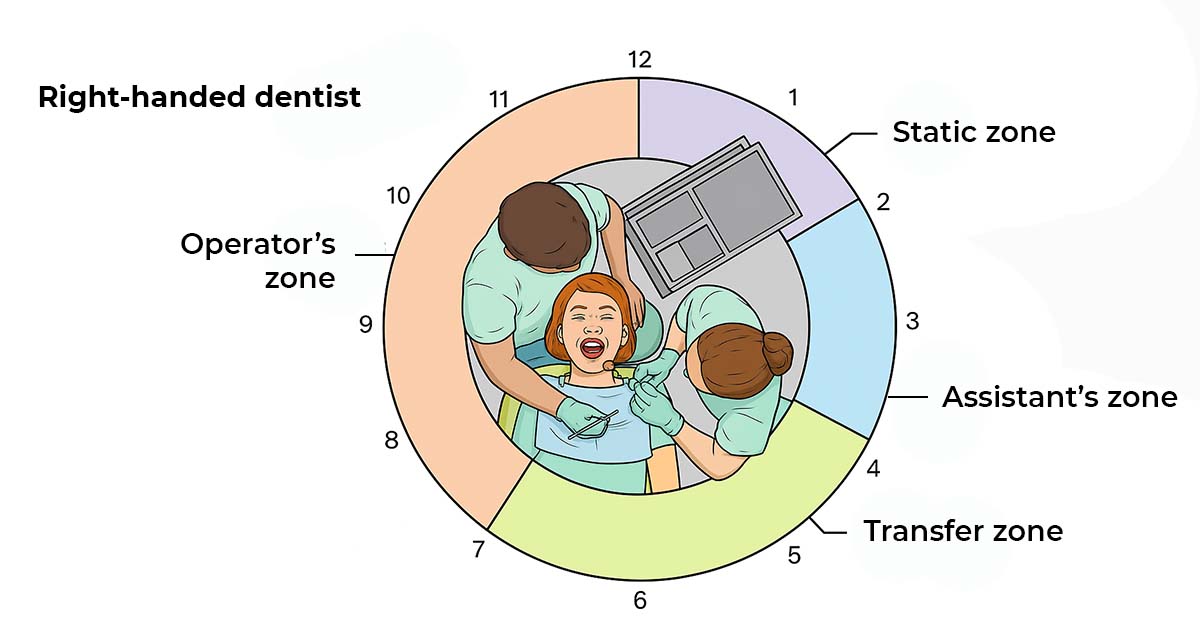
An assistant’s addition in a dental procedure helps to practice four-handed dentistry easily. It makes the dental procedure more comfortable, less exhausting, more stable, and helps in delivering more accurate and efficient treatment. The following are some basic rules that should be followed when practicing four-handed dentistry:
- The assistant sits on the left side, i.e., opposite the dentist, facing him directly. The working area for the assistant, with a cabinet, should be on the right side so that he can help in handing over materials and instruments as and when required.
- The dentist uses indirect visualization with a mouth mirror to allow the assistant to achieve improved direct visualization and avoid any awkward positions.
Thus, the assistant does not interfere with the dentist’s movement between the 7 o’clock and 12 o’clock positions. The operating field is clearly visible to both the operator and assistant, and the assistant also has direct access to the oral cavity. Instruments can further be handed over to the operator easily without hindering the procedure.
Optimal assistant seating allows easier access and proximity to the patient. The assistant should be seated on a stool so that his or her eyes are 15–20 cm higher than the dentist’s eyes. The stool should have foot support to allow the assistant to work both within and outside the oral cavity.
Instrument Exchange and Magnification:
Any instrument exchange between the operator and assistant should occur in the exchange zone—below the patient’s chin and a few inches above the patient’s chest. Instrument exchange should be strictly avoided over the patient’s face. During the procedure, the operator should inform the assistant in advance about the next required instrument to facilitate easy and continuous exchange.
The operator should try not to look away from the operating field and can rotate the instrument handle forward to cue the assistant for the exchange. The assistant should take the instrument from the operator, and the operator should ensure that the assistant has a firm grip before releasing it, and vice versa.
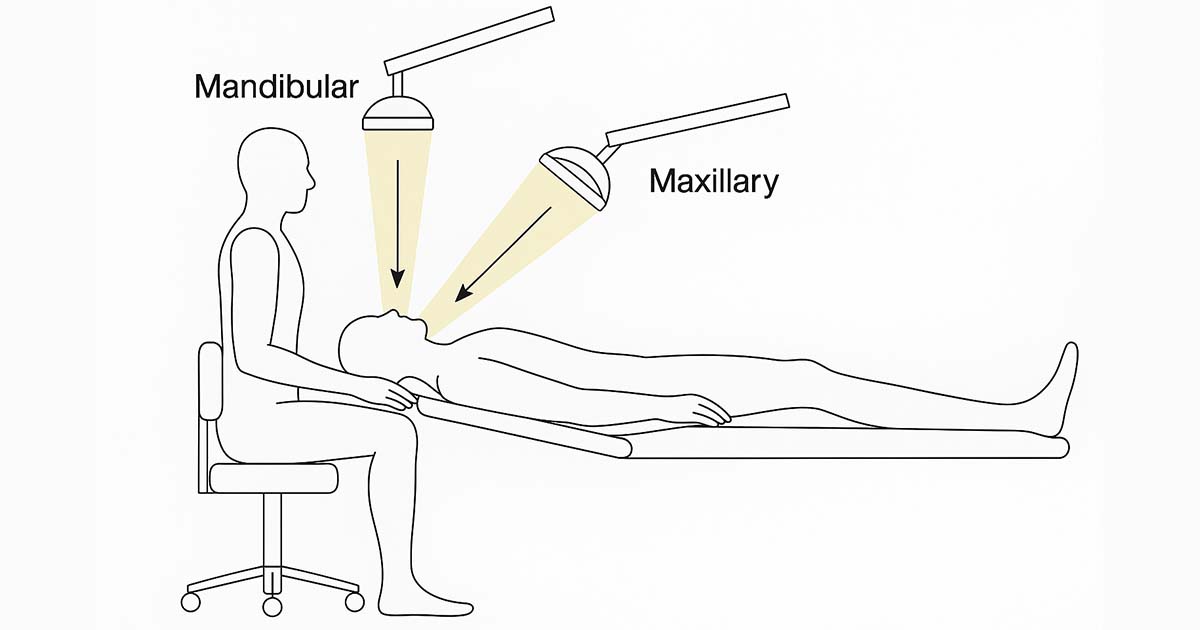
At all times, it is important that the operator has a clear view of the field of operation. Proper magnification—using loupes, indirect vision through a mouth mirror, and appropriate illumination—helps maintain visibility and precision. Headlamps aligned parallel to the clinician’s line of sight can eliminate shadows in the operating area, further enhancing visibility and control.
Conclusion:
Implementing proper dental ergonomics is essential for every dental professional to work efficiently and maintain long-term health. By adopting the ideal posture, ensuring correct patient and chair positioning, and practicing effective four-handed dentistry, dentists can minimize physical strain and fatigue. These ergonomic practices not only support the dentist’s well-being but also enhance precision and comfort during procedures. Prioritizing these principles helps create a safer, more productive environment, ultimately benefiting both the dental team and the patient.
No Comment